반응형
- 외상 후 심한 출혈에 의한 사망률은 30~40%. 외상 후 24시간 이내 사망 원인의 50% 차지
- Traumatic shock 환자에서 fluid & blood resuscitation 목적
Pathophysiology
- Hemorrhagic shock은 intravascular volume과 perfusion을 유지하기 위한 생리적 보상 작용 유발
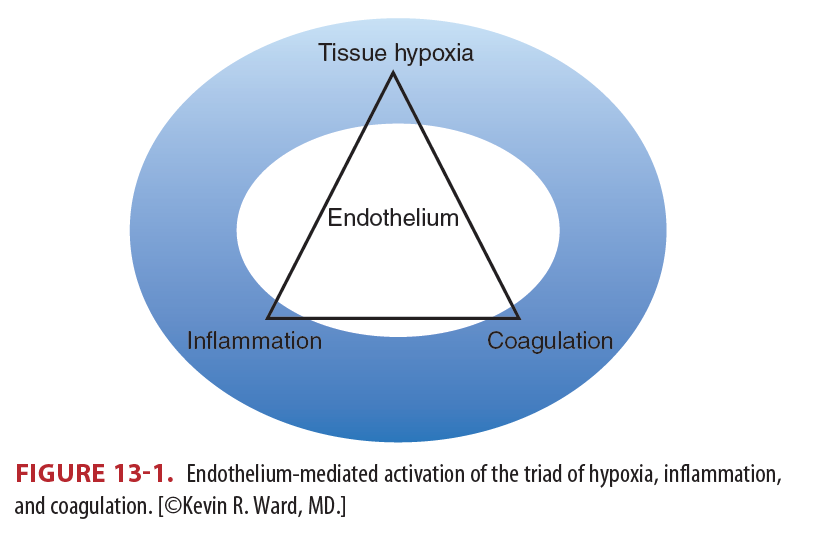
- Shock은 Vascular endothelium 손상 유발 → 응고와 염증을 일으킴 → 지속되는 경우 장기부전 발생
- Trauma-induced coagulopathy
Clinical features
- Hemodynamic response to acute severe hemorrhage-induced hypovolemia
- 평소 건강했던 사람은 실혈량이 많더라도 적극적인 생리적 보상 반응에 의해 위에서 언급한 반응이 보이지 않을 수 있음
- 노인의 경우에는 기저 심질환, β-blockers 같은 약물로 인해 tachycardia를 보이지 않을 수 있음
- 복부 출혈환자는 hemoperitoneum으로 인한 vagal tone의 상승으로 bradycardia가 생기거나 tachycardia가 생기지 않을 수 있음 (30% 정도)
- SBP, HR, GCS로 출혈의 중증도를 분류하는 방법은 신뢰할 수 없음
Diagnosis
- Severe hemorrhage를 파악하고 적절한 치료를 하는데 있어 V/S은 극단적인 상황이 아니면 가치가 적음. metabolic information, injury mechanism, imaging w/u 등이 도움
- early findings : Mixed or central venous hemoglobin oxygen saturation
- late findings : Lactate, base deficit
- Shock에서 lactate는 oxygen debt를 의미하지만 resuscitation 과정에서 lactate의 clearance가 resolution of oxygen debt를 의미하지는 않음
- (invasive) central venous oxygen saturation (ScvO2) measurement, (noninvasive) tissue oxygen saturation (StO2) measeurement 이용해 oxygen consumption을 연속적으로 측정할 수 있으며, 이를 60% ~ 70% 유지해야 tissue hypoxia 해결 가능
Treatment
Prehospital에서 치료의 우선순위
- Adequate ventilation and oxygenation
- Controlling external bleeding
- Protecting the spinal cord
ED에서 치료
- Restore intravascular volume
- Maintain oxygen-carrying capacity
- Limit ongoing blood loss
- Prevent the development of coagulopathy
Endo/exogenous cause → hypothermia
- 환자를 따뜻하게 하고 warmed IV fluids, blood products 주입 필요
Airway control, ventilation, and oxygenation
- PaO2 ≥ 94%
- pneumothorax, tension pneumothroax, hemothorax, upper airway obstruction 등을 파악
Vascular access and monitoring
- Large-bore (14- to 16-gauge in adults) peripheral lines, two or more
- Monitoring ECG, pulse oximetry, ETCO2
- Check arterial blood pressure, mental status, peripheral perfusion
- Bedside FAST, POCUS
Hemostatic-hypotensive resuscitation
- 지나친 volume expansion과 blood pressure 정상화는 hemorrhage 악화
- Hypotensive resuscitation : surgical bleeding control 가능한 시점까지 SBP를 허용 가능한 수준에서 유지하면서 initial fluid resuscitation을 제한. 일반적으로 SBP 90mmHg 정도로 보지만 뚜렷한 evidence 없음
- Myocardial disease, cerebral ischemia, or traumatic brain injury 환자에서는 금기
Isotonic crystalloid solutions
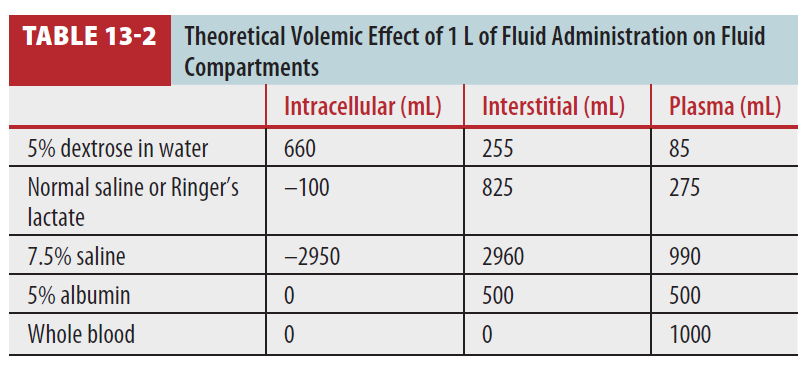
- Isotonic crystalloids : hypo-oncotic → 70%가 extravascular space로 빠져나감. intravascular volume replacement 하려면 출혈량의 3배 필요.
- Isotonic crystalloids 다량으로 사용할 경우 아래의 문제
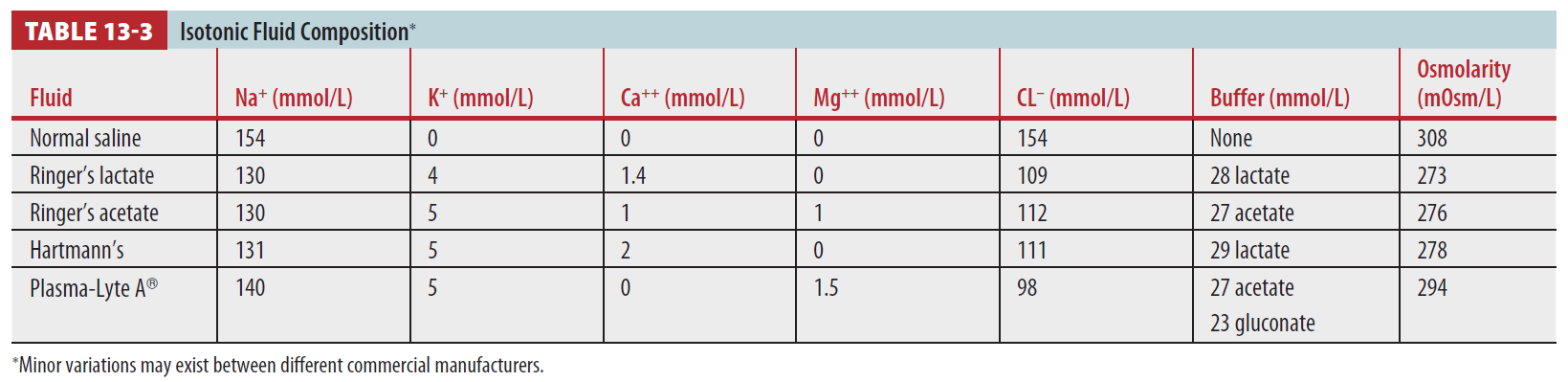
- Balanced crystalloids : Lactate 또는 acetate 포함하고 있는 solution. buffer 포함. Cl 적게 포함. NS에 비해 clinical outcome 좋음
Colloid solutions
- Crystalloids에 비해 oncotic pressure 높아 적은 volume으로 hemodynamic goals 달성할 수 있으나, traumatic shock에서 mortality 및 morbidity 감소가 입증된 바 없음
- 감소된 Hb 회복시켜 줄 수 있지만, plasma, platelets 없이 pRBC만 보충해준다고 hemostasis가 촉진되거나 tissue oxygenation이 완전히 회복되지는 않음
- 출혈이 완전히 control된 경우 Hb >7 g/dL면 수혈하지 말 것
- CAD, CVD 있는 환자의 경우에도 일반적으로 Hb >10 g/dL면 수혈로 얻을 수 있는 이점이 없음
Plasma
- FFP은 모든 응고인자를 포함하고 있으며 1 unit은 200-250mL
Platelets
- PC 6 unit 또는 apheresis-collected single-donor platelet concentrate 1 unit은 성인에서 platelet count 50,000/mm3 가량 상승시킴
Massive transfusion protocols
Concept
- 보통 외상 후 24시간 이내에 10 units 이상의 pRBC를 수혈 뜻함
- ABC score (The Assessment of Blood Consumption)
Protocol
- High plasma-to-pRBC ratio resuscitation : 응고장애의 유무와 무관하게 survival benefit 있음 (1:1.4 > 1.18, 1.25)
- Plasma : Endothelial repair, reducing vascular permeability → Cell survival 증가 → Perfusion과 Tissue oxygenation 개선
- Platelets 함께 보충하는 것은 clinical outcomes, mortality, blood loss에 benefit 있음
- Institution-specific massive transfusion protocol 권장
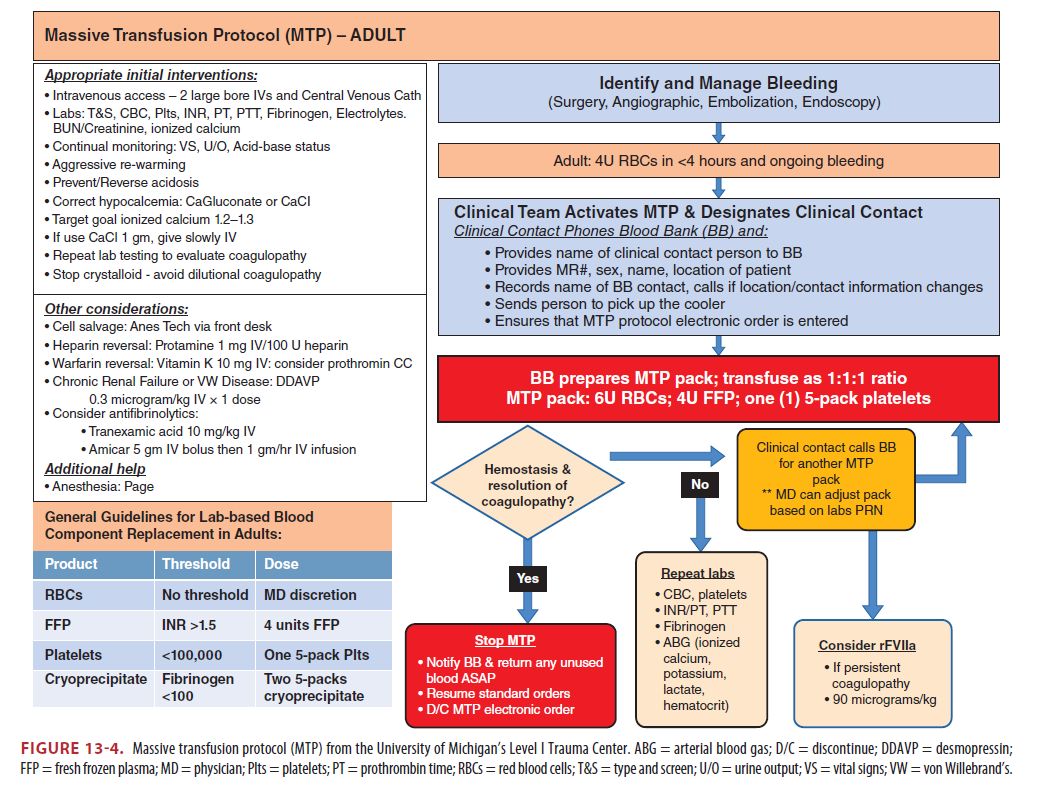
Adjuncts
- Tranexamic acid (antifibrinolytic)은 major trauma 환자에서 resuscitation의 초기에 사용할 경우 improved survival, reduces overall mortality 입증
- pRBC, FFP는 citrate 포함하고 있음 → calcium과 결합하여 life-threatening hypocalcemia 유발 : Ca2+ 보충(calcium chloride 선호) 및 ionized calcium monitoring(>0.9mmol/L)
Reference
Tintinalli's Emergency Medicine, 9th, chapter 13, p.63~68
반응형
'의학자료 > Resuscitation' 카테고리의 다른 글
| 알러지 및 아나필락시스 Allergy and Anaphylaxis (0) | 2022.12.21 |
|---|---|
| 비외상성 쇼크 Nontraumatic shock (0) | 2022.12.18 |





