반응형
Epidemiology
- 병원 사망률 : Septic shock 26%. cardiogenic shock 39%-48%
- Spine cord injury → Neurogenic shock <20% (Cervical 19.3%, Thoracic, 7%, Lumbar, 3%)
- Evaluation, treatment, stabilization 동시에 할 것
Pathophysiology
- Shock :순환부전으로 tissue oxygen supply and demand의 불균형이 나타나 end-organ dysfunction이 발생하는 것
- 4 categories : (1) Hypovolemic (2) Distributive (3) Cardiogenic (4) Obstructive
(1) Hypovolemic shock
- Intravascular fluid 감소 → preload, stroke volume, cardiac output(CO) 감소
- Severe blood loss → myocardial oxygenation 감소 → contractility, CO 감소
- autonomic increase → systemic vascular resistance(SVR) 상승
(2) Distributive shock
- Systemic vasodilation → 상대적 intravascular volume 부족
- Septic shock에서 가장 흔함
- SVR 감소 → 보상 반응으로 CO (contractility, HR) 상승하나 preload 감소로 인해 상쇄
- Sepsis 환자 40% 정도가 transient cardiomyopathy → 수축력 감소하고 사망률 증가
- septic shock 외에 Anaphylaxis, adrenal insufficiency, neurogenic shock
(3) Cardiogenic shock
- LV failure (contractility, preload, afterload, right ventricular function 등 영향) → oxygenated blood가 peripheral tissue로 전달되지 않는 경우
- 원인은 대부분 MI (m/c), dysrhythmias. 이후 infection이 동반되는 경우가 많음
(4) Obstructive shock
- uncommon (1%)
- Venous return 이나 cardiac compliance가 감소
- 원인은 Cardiac tamponade, pulmonary embolism, tension pneumothorax 등

Factors affecting cardiac output
- CO는 HR과 stroke volume으로 결정
- Stroke volume은 reload, afterload, contractility로 결정
- MAP는 CO와 SVR로 결정 : SVR는 직접적으로 arterial pressure에 영향을 주기도 하지만 afterload에 영향을 줘서 결과적으로 CO에 영향
- CO는 심장의 3가지 성질의 상호작용으로 결정 (Chronotropy and Lusitropy 모두 교감신경에 자극 받음)
- Shock states에선 고농도의 epinephrine 배출 → adrenergic tone 강화
Lactic acid
- Tissue supply & demand imbalance에 대한 보상작용이 부족할 경우 anaerobic metabolism → lactic acid 상승
- 대부분의 lactic acidosis는 부적절한 산소 공급으로 발생
- Lactate 상승은 중증 환자들의 단기 예후 예측에 도움
- Serial lactate f/u 필요. Lactate clearance는 septic shock에서 좋은 예후와 연관
Compensatory mechanisms and their failure
- Shock → autonomic response → Vital organ perfusion pressure 유지
- Carotid baroreceptor 자극은 아래와 같은 방식으로 sympathetic nervous system 반응 유발
- 보상작용은 Critical organ (heart, brain) 산소공급 유지. Kidneys, GI tract 등의 공급 저하
- Oxygen delivery 저하 → 세포에서 ion-pump dysfunction 발생 → Na+ 유입, K+ 배출, membrane resting potential 감소
- Shock 진행됨에 따라 cellular homeostasis 무너지고 hyperkalemia, hyponatremia, azotemia, hyper- or hypoglycemia, lactic acidosis 등 유발
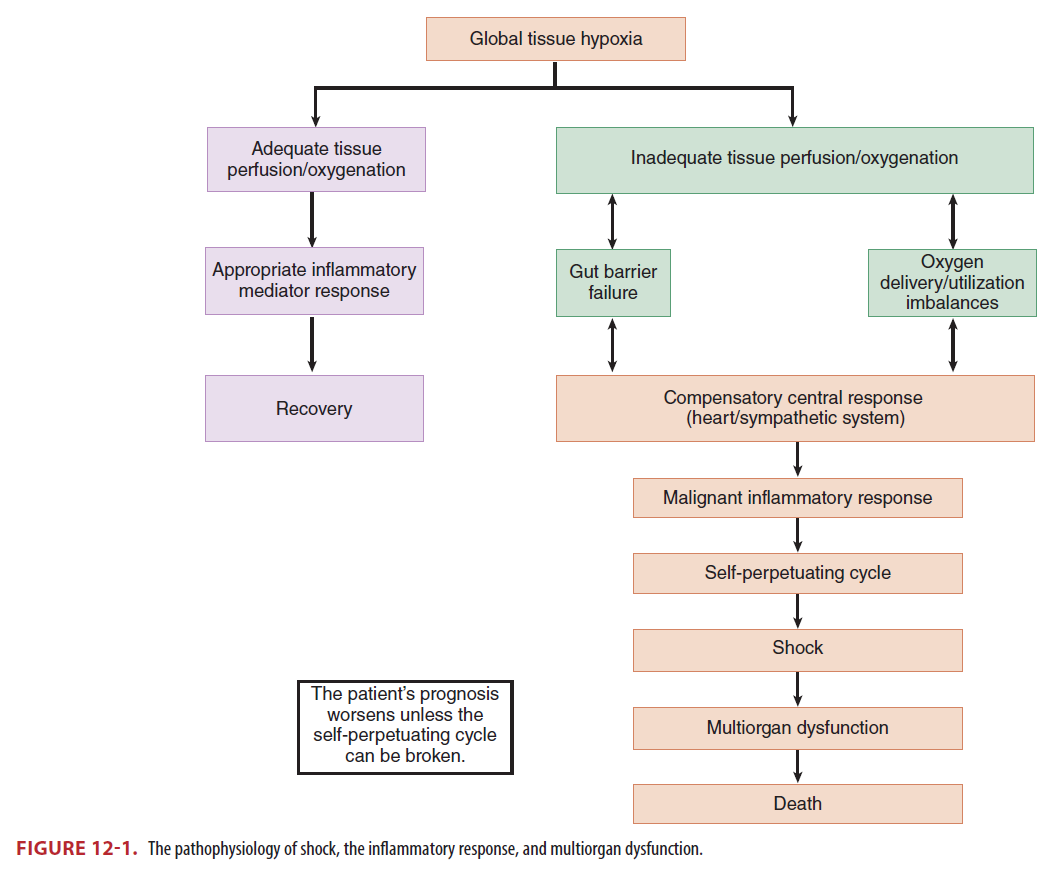
- Global tissue hypoxia 진행되면 multiorgan dysfunction syndrome 발생
Clinical features
History & comorbidities
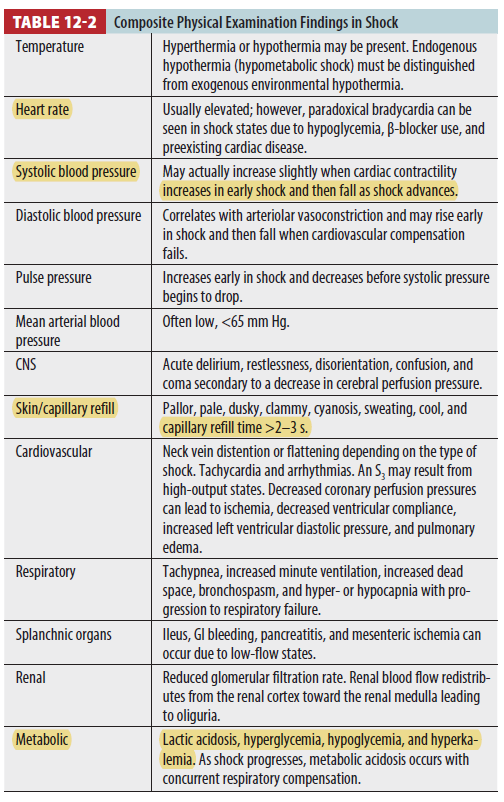
Physical examination
- 환자에게 직접 Hx 하기 어려울 수 있어 EMS, 가족 등의 정보를 활용
- 환자가 반응이 없을 시에는 trauma를 꼭 염두해 두자!
- 대부분의 shock은 systemic arterial hypotension (SBP<90mmHg)을 동반함
- SVR 증가하여 BP는 정상이지만 tissue hypoperfusion 발생 가능 → BP로 global tissue hypoperfusion 민감하게 판단할 수 없음. peripheral vascular disease, tachycardia with a small pulse pressure, cardiac dysrhythmias 동반된 경우 BP는 민감도가 더 떨어짐
- Shock may occur with a normal blood pressure, and hypotension may occur without shock
- 따라서 여러 임상양상을 종합해서 shock 여부를 판단해야 함
Diagnosis
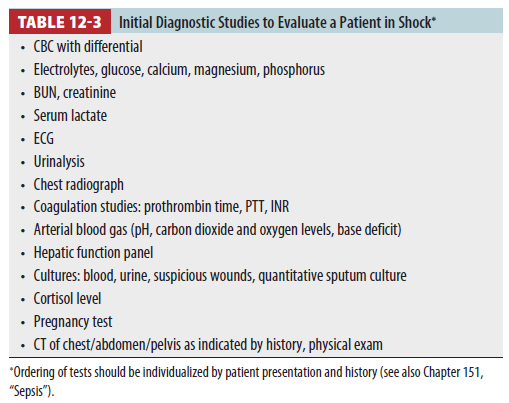
Laboratory evaluation
- No single laboratory value is sensitive or specific for shock
- ABGA는 acid-base status와 ventilation, oxygenation 평가에 유용
- Serum lactate 상승은 mortality와 연관
Imaging
- CXR : heart size, presence of pulmonary edema, pneumothorax, infiltrates, effusion, free air
- US : volume status, defining cardiac function 등 평가.
- CT : Unstable shock에서 촬영 어려움. renal function 고려 (hypovolemia, contrast induced nephropathy)
Hemodynamic monitoring
- Severity 평가하고 치료에 반응하는지 확인
- Critical 할 경우 intra-arterial blood pressure monitoring, end-tidal CO2 monitoring, CVP, ScvO2 측정
- procedure complication 줄이기 위해 intervention시 초음파 사용 권장
Treatment
* hemodynamic end point with early goal-directed therapy 시행한 경우 사망률 16% 감소
* ABCDE bundle : Airway, controlling the work of Breathing, optimizing the Circulation, ensuring adequate oxygen Delivery, and achieving End points of resuscitation
Establishing the Airway
- Airway control 가장 확실한 방법 Intubation
- Sedative → vasodilatation, or myocardial suppression → hypotension
- Positive-pressure ventilation → preload, CO 감소
- Sedative + Positive-pressure ventilation → hemodynamic collapse
- Intubation 하기 전에 최대한 resuscitation 할 것 (volume replacement, vasoactive agents)
Controlling the work of Breathing
- Work of breath가 매우 높은 경우 breathing control 필요
- Shock 상태에서 호흡근은 산소를 많이 소비하여 lactate 생성을 유발
- MV 시작하기 전에 compensatory minute ventilation 고려
- ARSD 같은 Severe hypoxemia 상태에서는 NMB 추가 고려
Optimizing the circulation
Fluids
- IV line 확보하면서 circulatory or hemodynamic stabilization 시작
- Trendelenburg position은 supine position에 비해 cardiopulmonary perfomance를 향상시키지 못함. 오히려 gas exchange를 악화시키고 aspiration 위험을 높임
- Passive leg raising은 효과적. → BP, CO 상승 소견 있으면 fluid resuscitation 필요
- Fluid resuscitation은 isotonic crystalloid로 시작하며 balanced crystalloid(HS)가 NS 보다 약간의 생존률 이득이 있음 (14.3% vs. 15.4%)
- 대부분의 septic shock 환자는 absolute or relative volume deficit 존재.
- 초기 5-20분 동안 500~1000mL NS bolus 공급하고 다시 평가.
- Modest hypovolemia 환자에서는 20-30mL/kg NS (sepsis guidelines에선 초기 30mL/kg)
- Profound hypovolemia 환자에서는 fluid를 더 주어야 하며 24시간 내 6L hydration 하는 경우도 흔함
- NS는 hyperchloremic metabolic acidosis 유발 → lactated Ringer’s or Plasma-Lyte 고려
- C-line은 volume status, ScvO2 평가할 수 있고 vasopressor 사용할 수 있어 도움
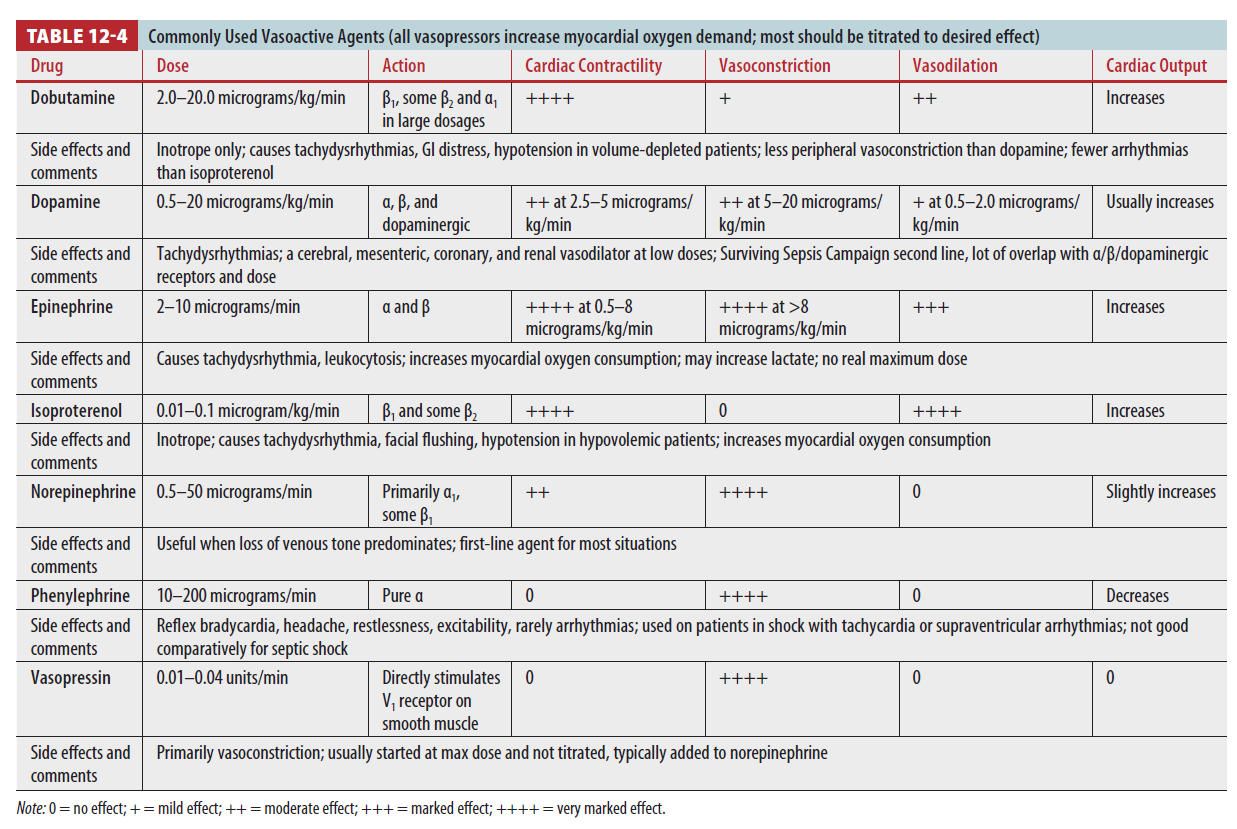
Vasopressors
- Volume resuscitation에 효과가 없거나 volume infusion 불가할 경우 사용
- Vasopressor는 volume 충분할 경우 효과가 있음 (volume replacement 충분히 한 후 사용)
- Chronic hypertension 환자는 저혈압 시 renal injury 위험이 증가
- MAP 65~70mmHg 이상 올리는 것은 생존율에 이득이 없음
- Vasopressor는 large vessels perfusion 늘리나 tissue bed의 capillary blood flow 감소 (특히 GI tract, peripheral vasculature)
- Vasopressor와 함께 inotrope을 써야하는 경우도 있음 (contractility, SV 증가 → CO 증가)
Ensuring adequate oxygen delivery
- Shock, pain, stress 등으로 hyperadrenergic state 유발
- 통증은 산소 공급을 줄이고 소모를 늘려 심근기능을 약화 → 통증조절 중요함!
- Arterial oxygen saturation ≥91%, Hb≥7g/dL
- Lactate, Svo2 or Scvo2 순차적 검사는 환자의 resuscitation 평가할 수 있는 방법
End points of resuscitation
- MAP > 65 mmHg
- CVP 8~12 mmHg
- Scvo2 > 70%
- Urine output > 0.5mL/kg/hr
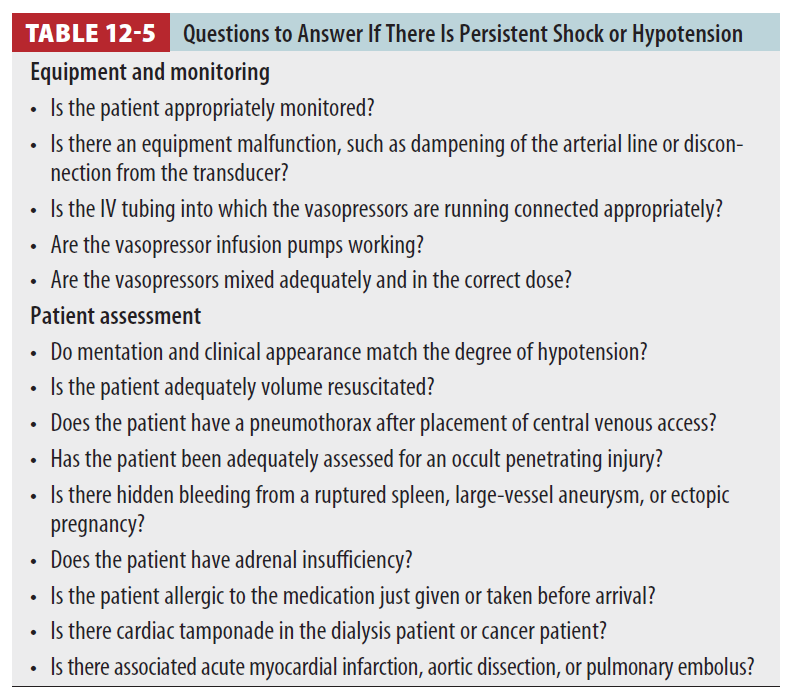
- source control 이 가장 중요하며 Shock 지속될 때 아래의 질문들에 답해볼 것
Reference
Tintinalli's Emergency Medicine, 9th, chapter 12, p.57~63
반응형
'의학자료 > Resuscitation' 카테고리의 다른 글
| 알러지 및 아나필락시스 Allergy and Anaphylaxis (0) | 2022.12.21 |
|---|---|
| 외상성 쇼크 Traumatic shock (0) | 2022.12.19 |





